A brain aneurysm is or ballooning in a blood vessel in the brain, usually caused by a weakness in the vessel wall.. It often looks like a berry and are also called berry aneurysms.
A brain aneurysm can rupture, causing bleeding into the brain (hemorrhagic stroke). Most often a ruptured brain aneurysm occurs in the space between the brain and the thin tissues covering the brain. This type of hemorrhagic stroke is called a subarachnoid hemorrhage.
The annual rate of rupture is approximately 8 – 10 per 1,00,000 people. Ruptured brain aneurysms are fatal in about 40% of cases. Of those who survive, about 66% suffer some permanent neurological deficit.
Approximately 15% of patients with aneurysmal subarachnoid hemorrhage (SAH) die before reaching the hospital. Most of the deaths from subarachnoid hemorrhage are due to rapid and massive brain injury from the initial bleeding which is not correctable by medical and surgical interventions. 4 out of 7 people who recover from a ruptured brain aneurysm will have disabilities.
Brain aneurysms are most prevalent in people ages 35 – 60, but can occur in children as well. The median age when aneurysmal hemorrhagic stroke occurs is 50 years old and there are typically no warning signs. Most aneurysms develop after the age of 40.
Most aneurysms are small, about 1/8 inch to nearly one inch, and an estimated 50 to 80 percent of all aneurysms do not rupture during the course of a person’s lifetime. Aneurysms larger than one inch are referred to as “giant” aneurysms and can pose a particularly high risk and can be difficult to treat.
Women, more than men, suffer from brain aneurysms at a ratio of 3:2.
Ruptured brain aneurysms account for 3 – 5% of all new strokes.
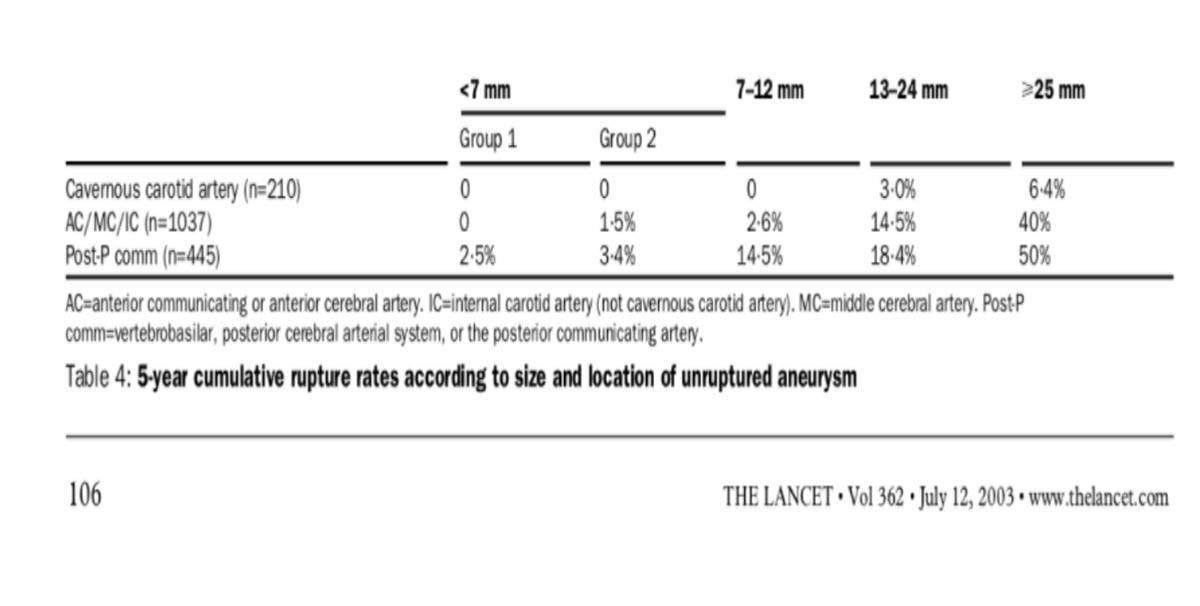
Subarachnoid hemorrhage (SAH) is one of the most feared causes of acute headache upon presentation to the emergency department. Treatment for an unruptured brain aneurysm may be appropriate in some cases and may prevent a rupture in the future. The ISUIA-1 and ISUIA-2 study provided an estimate of risk rupture for these unbled aneurysm.
The table taken from the Lancet publication below provided below gives an estimate of risk of rupture.
Symptoms
Ruptured aneurysm
A sudden, severe headache is the key symptom of a ruptured aneurysm. This headache is often described as the “worst headache” ever experienced.
Common signs and symptoms of a ruptured aneurysm include:
Sudden, extremely severe headache- a thunderclap headache.
Nausea and vomiting
Stiff neck
Blurred or double vision
Sensitivity to light
Seizure
A drooping eyelid
Loss of consciousness
Unruptured aneurysm
An unruptured brain aneurysm may produce no symptoms, particularly if it’s small. However, a larger unruptured aneurysm may press on brain tissues and nerves, possibly causing:
Pain above and behind one eye
A dilated pupil
Change in vision or double vision
Numbness of one side of the face
Management of the aneurysm:
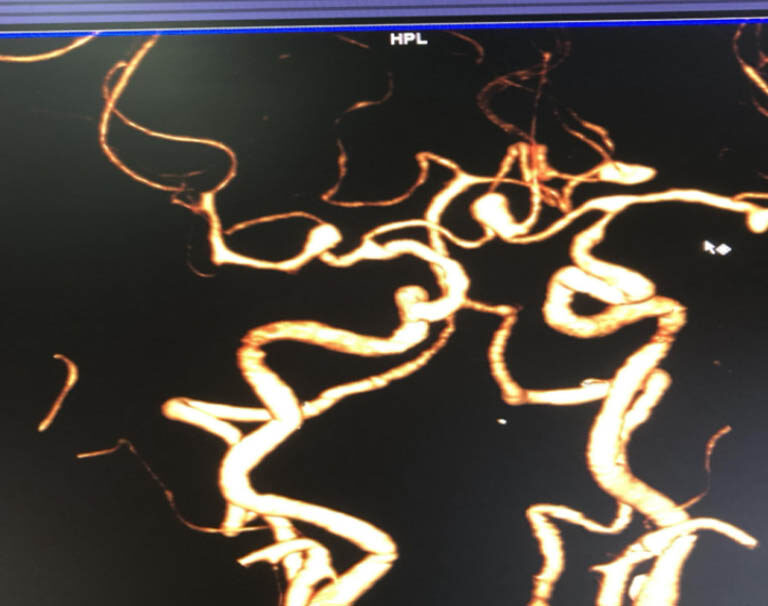
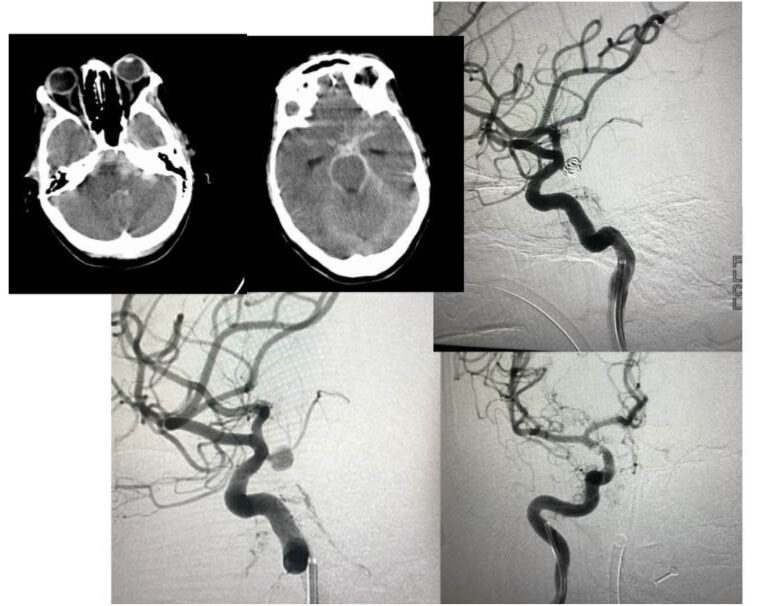
Ruptured aneurysms are diagnosed with radiological imaging such as MR imaging and CT angiography. A diagnostic cerebral angiogram, which is a gold standard may be needed at times to delineate a small aneurysm or to better qualify its morphology and plan treatment.
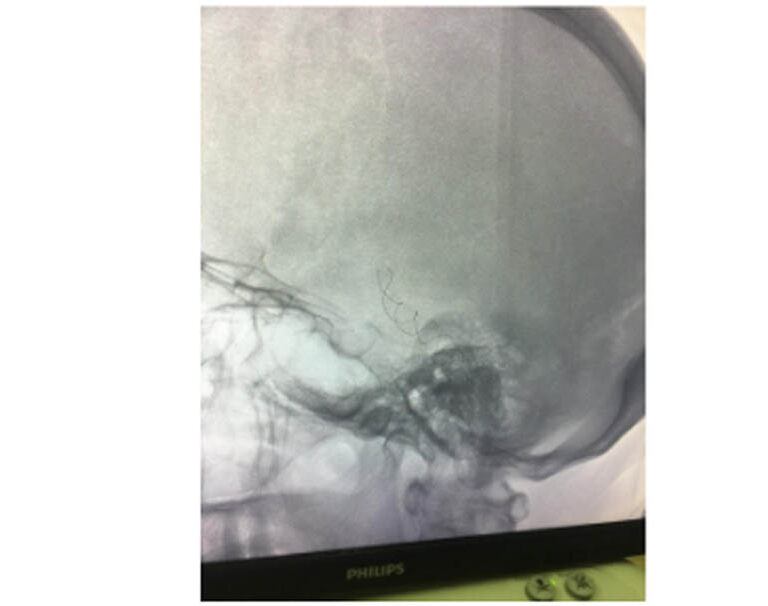
CT head showing subarachnoid haemorrhage and intraventricular haemorrhage
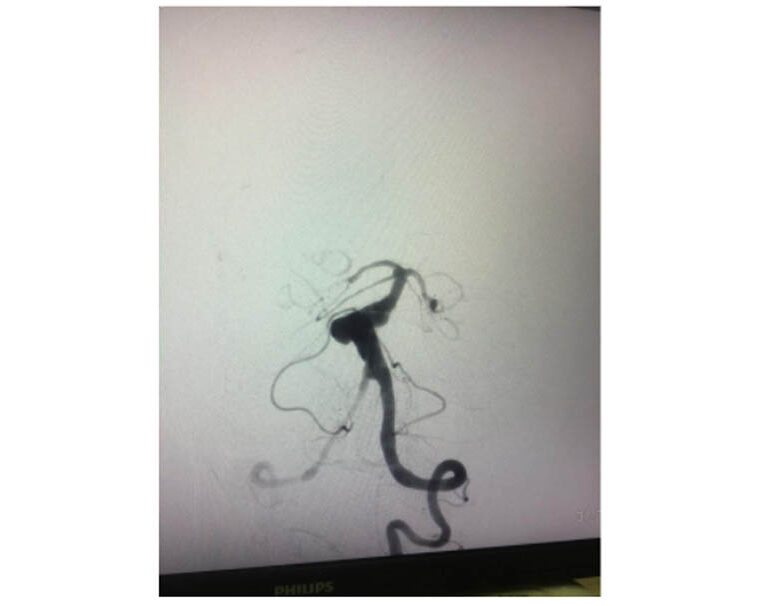
CT angiogram showing 4 aneurysms in a patient
Management of saccular aneurysms:
Management of saccular aneurysm is with either surgery- clipping of the aneurysm or endovascular coiling of the aneurysm.
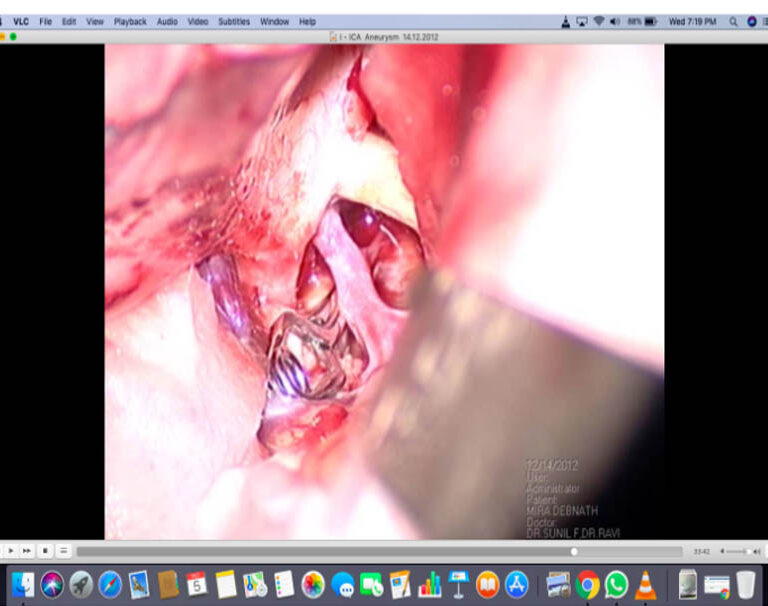
Surgery:
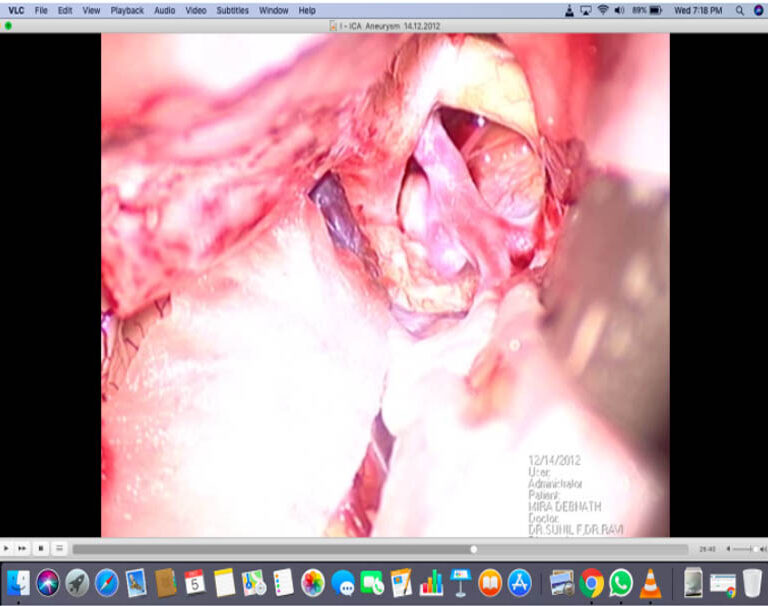
Surgery involves creating a window on the skull, retracting the brain gently, identifying the aneurysm and placing clip to occlude the aneurysm from the circulation
Exposed PCOM aneurysm which is ready for surgical clipping.
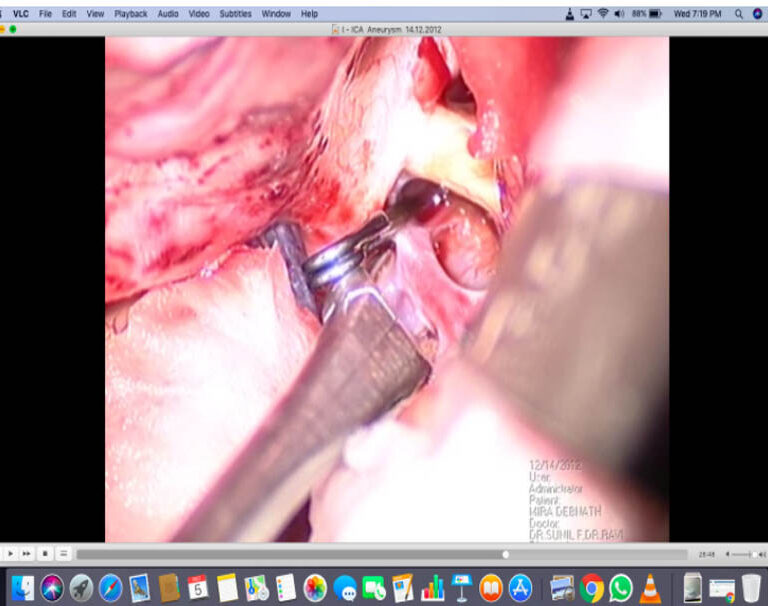
Appropriate clip placed across the aneurysm
Aneurysm clipped and excluded from the circulation to prevent a re-bleed
Coiling of aneurysms:
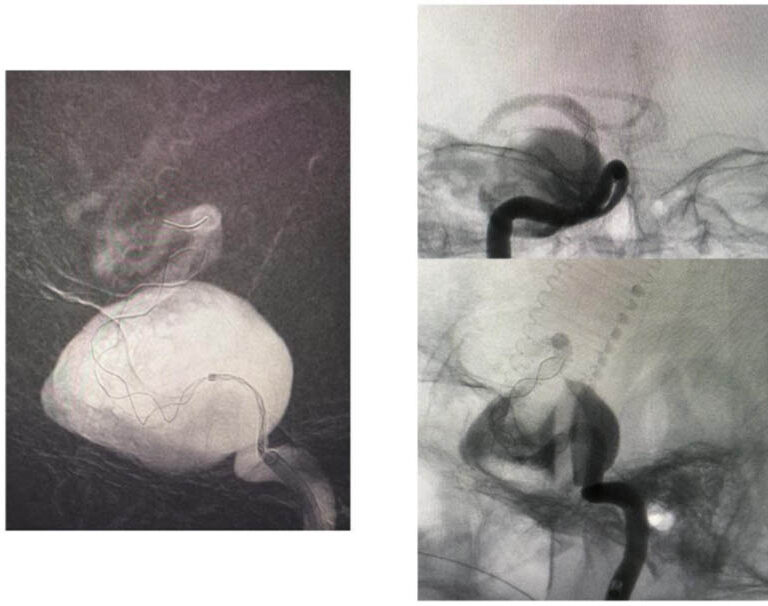
Saccular aneurysms can be coiled as a method of treatment. However, we may need to use special devices like a protective intracranial balloon or stent while coiling in order to keep the coils within the aneurysm during and after the procedure.
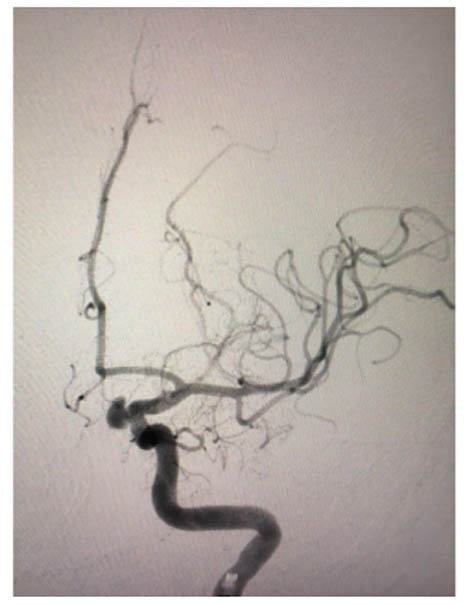
Pre-Coiling of superior hypophyseal aneurysm
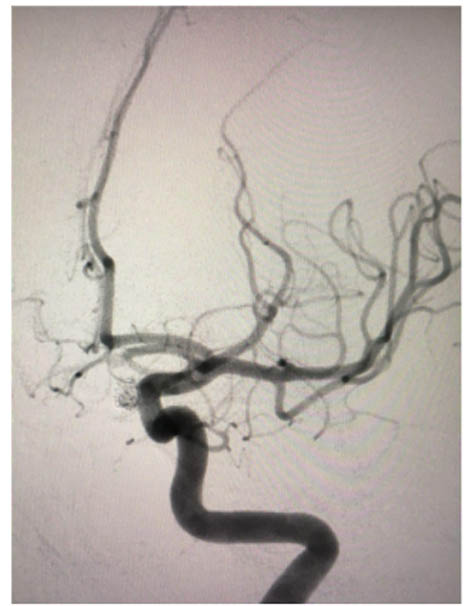
Post-coiling of superior hypophyseal aneurysm
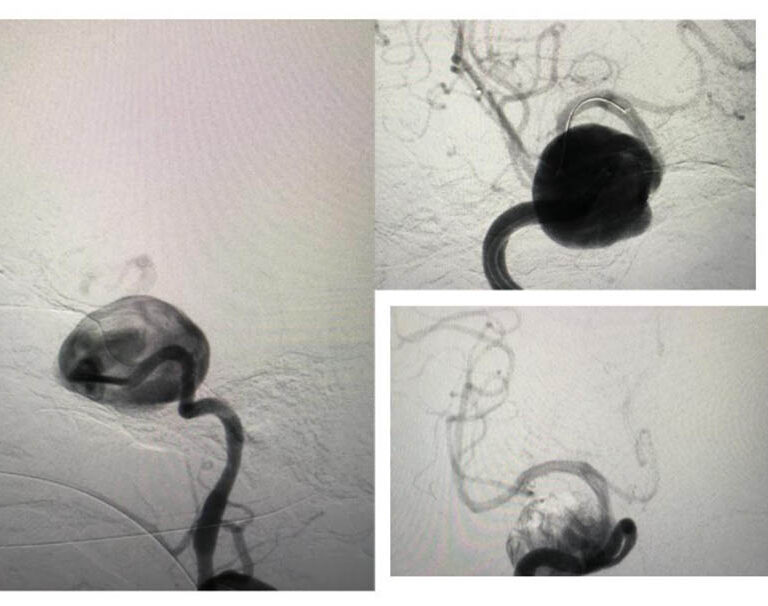
Coiled posterior communicating segment aneurysm
Giant cavernous segment aneurysm
Flow diverter placement done for the giant cavernous segment aneurysm
Giant aneurysms in the intracranial circulation are best treated by flow diverter placement as shown above.
Fusiform aneurysms:
These are dilatation in the vessel wall either due to it being inflamed or due to atherosclerotic disease
They are best managed by endovascular methods like flow diversion using special stents.